
How I Fixed Mild Obstructive Sleep Apnea And Transformed My Face In My Late 20s
Mar 27, 2023
You are about to embark on a journey through my personal experiences with sleep, breathing and performance problems over the last few years that have culminated in the Breathe Sleep Perform Program.
This is not the shortest blog post you'll ever read, but it may save you thousands of dollars, years of pain, frustration and suboptimal performance due to poor sleep.
The information contained herein is NOT medical advice, nor should it be used to diagnose any medical conditions. It is a 100% unfiltered true story of my life.
![]()
Where It All Started - 2018 - 25 Years Old
I used to wake up each day grumpy and exhausted, even after spending 8 hours in bed.
My sleep quality was terrible.
I was a loud snorer. I tossed and turned and often woke up from a pool of sweat. I got up to the toilet at least twice a night.
My girlfriend (now fiance, luckily), Theresa, told me that sometimes my snoring was interspersed by a few large gasps for air. It was almost as if I couldn't breathe.
My restless sleep kept her up at night.
Or so she thought, but it turns out she was going through nightly struggles of her own.
See, Theresa had suffered from severe dust allergies for her whole life. She told me she'd been on a nasal decongestant for as long as she could remember.
Her breathing would be audible as the air whistled through the small gaps of air between what sounded like barrages of mucous. It drove me crazy.
After a while, since we moved in together in 2018, we both woke up grumpy and ready to complain and attack each other about trivial things.
Our sleep problems were seriously testing our relationship. I was second-guessing my decision to stay in Australia and create a life with her.
This time was also the first time I experienced any form of anxiety. I found it weird because I've always been very confident and found it easy to spend time alone.
I could not focus on cognitively challenging tasks for very long, especially in the afternoons.
I wasn't recovering properly from my training, and I knew I couldn't train as hard as I wanted to.
Probably the MOST alarming thing was that my libido wasn't the same as it used to be. I didn't feel like it as often as I used to, and with the same intensity.
All this was very alarming because I was 25 years old and was supposed to be in my prime.
None of this made sense because I was fit and consistent like a soldier with my sleep hygiene regime.
See, I had already been a personal trainer for a few years, and one of the things required to be a successful personal trainer is that you must be well-versed in the physiology of sleep to be able to troubleshoot and assist your clients in improving their sleep quality.
Sleep is essential for mental and physical health. Sleep deprivation has also been proven to impair the body's ability to lose body fat even while in a calorie deficit. (Nedeltcheva et al 2010)
You'll lose more muscle and less body fat, and it will be harder to stick to your diet if you don't sleep enough. And beyond that, you won't be able to push yourself hard enough at the gym if you aren't getting uninterrupted sleep at night. A recipe for disaster if your goal is to improve how you look naked.
That's why I had already spent considerable time researching all the possible sleep hygiene considerations known to man. I knew about the importance of a solid circadian rhythm, optimal light exposure, the impact of chronic stress, caffeine, and the importance of a cold and dark sleeping environment and, many other things.
Being more mindful of our sleep hygiene helped. However, both I and Theresa knew that things could be better.
I wasn't sleeping properly, and this was having a severe negative impact on the quality of my life.
I also knew that it would severely impact the QUANTITY of my life, as chronic sleep deprivation has been linked to a shorter lifespan.
I knew that I had to do something. I kept researching, and one day I found something.
Oxygen Advantage
One day I was on a walk listening to a favourite podcast of mine, which featured Patrick McKeown, the world's foremost health and performance breathing expert.
Patrick took the listeners through a simple but powerful exercise designed to reduce stress immediately and improve habitual breathing.
The first time I tried slowing down my breathing and reducing the amount of air I was breathing while breathing exclusively through my nose, I immediately realised that there was something here that I'd never heard of before.
A whole can of worms waiting to be cracked open.
I ordered Patrick's book, The Oxygen Advantage, later that same day.
I learned about the importance of carbon dioxide tolerance for sleep quality and general health. It turns out that carbon dioxide is not just a waste gas when it comes to breathing. Your tolerance to carbon dioxide, determined by your chemoreceptor sensitivity, dictates how deep, shallow, regular or irregular your breathing is. This, in turn, influences how deep or shallow your sleep is and how easy it is for you to wake up.
I was thrilled to learn that carbon dioxide tolerance was something that you could train with specific breathing exercises that could be performed anywhere, anytime, by anyone without any equipment.
The other thing about these exercises is that they quieten the mind and allow you to achieve monk-like states of relaxation within minutes of practice.
After about a year of self-study and experimentation on the biochemistry and biomechanics of breathing, I completed Patrick's 3-Day Health And Sports Performance Breathing Instructor course and became a certified Oxygen Advantage Instructor in early 2020.
At this point, I had been practising the exercises daily and had noticed a profound positive change in the quality of my sleep.
I followed Patrick's advice religiously and spent 5-10 minutes on what I call Stress Relief Breathing (Covered in detail in the Breathe Sleep Perform Program) to prime my breathing to be light and through the nose while I slept.
I then placed a piece of sensitive skin tape across my mouth each night to ensure that my mouth stayed shut while I slept.
It turns out that mouth breathing during sleep increases arousal levels and the risk of snoring and obstructive sleep apnea.
Together my new breathing habits and mouth-taping were absolute game-changers.
And I wasn't the only one benefiting from these exercises. For the first time in my girlfriend's life, her nose wasn't blocked. That might sound basic, but for someone who's had to use a decongestant every day for as long as she can remember, that's absolutely huge.
See, one of the exercises that I teach in the Breathe Sleep Perform program, the "Nose Unblocking Exercise", naturally opens up even the most clogged-up nose in a matter of minutes.
Then, once that nose is open, it will stay open because the airflow itself will encourage the soft tissues of the nasal passages to yield and accommodate better airflow. Even better, because you are taking advantage of the nose's air filtration, humidification and warming qualities, your body doesn't produce excessive amounts of mucous in the first place.
The more you breathe through your nose, the easier it will become to breathe through your nose.
Becoming full-time nasal breathers was life-changing for both my girlfriend and me.
She could finally breathe easy, and I could finally rest my mind because I didn't have to listen to the air wheezing through the microscopic gaps in her nasal passages.
However, even though my sleep quality had improved dramatically due to better sleep hygiene and new breathing habits, I still woke up several times a night.
I had to keep searching.
A Trip To The Dentist
Through my research into sleep-disordered breathing, I realised that I had been a snorer because I used to breathe through my mouth and was used to breathing large quantities of air.
At this point, I had become a full-time nasal breather during the day and night, and my carbon dioxide tolerance had improved significantly (it was now easy for me to maintain nasal breathing while exercising at low and moderate intensities).
Since I was still experiencing some of the symptoms of obstructive sleep apnea (sleepiness, inability to focus, waking up frequently, night sweats, frequent urination, low libido, mood swings, and anxiety), I decided to do a sleep study.
I found a brilliant dentist in Melbourne who specialises in sleep-disordered breathing, Dr Damian Teo.
Dr Teo promptly prescribed me a sleep study, and the kit arrived at my home a few days later.
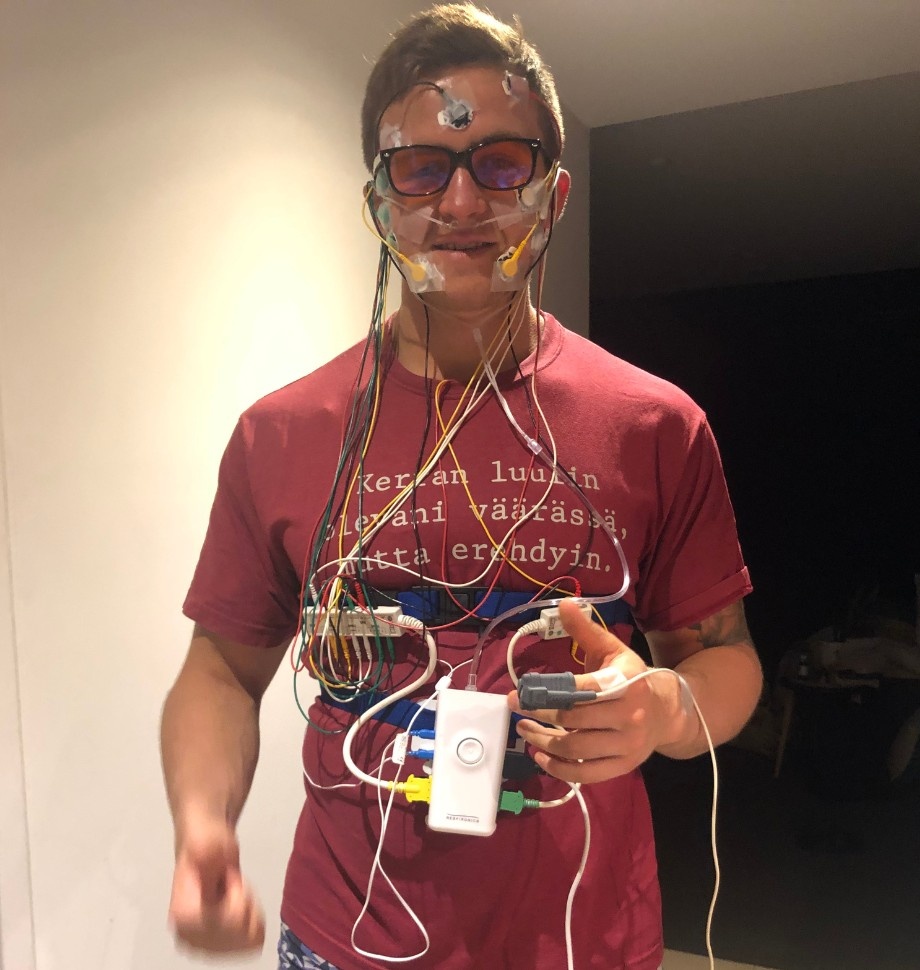
Wired Up And Ready To Go
Hands down, that was the worst night of my life. The wiring was so uncomfortable that I barely slept that night.
Dr Teo warned me this might be the case but reassured me that all they would need is a few hours of total sleep to get an idea of the quality of my breathing while I slept.
The results came the following week.
I woke up an average of five times per hour. That's the low threshold of mild obstructive sleep apnea.
Even though five wake-ups per hour sounds extreme, it's not.
0-5 Wake-ups per hour are considered "normal".
5-15 Wake-ups per hour are considered mild sleep apnea.
15-30 Wake-ups per hour is considered moderate sleep apnea.
30+ Wake-ups per hour is considered severe sleep apnea.
Holy cow. I only woke up an average of 5 times per hour, and I felt like crap. I knew I wasn't operating even close to my potential.
I can't even begin to fathom what people with moderate or severe sleep apnea are going through.
Dr Teo also did an orthodontic assessment, and he identified that the reason for my obstructive sleep apnea was that my tongue was too big for my mouth.
What?
How the hell is that possible?
Those were my initial thoughts, but then I remembered the ten excruciating years of orthodontics I underwent from age 5 to age 15.
See, I have a Class 3 malocclusion, also known as severe crossbite, meaning that my maxilla, the upper jaw, is underdeveloped compared to my mandible, the lower jaw.
The Finnish orthodontist who treated me tried expanding my maxilla but was never quite able to achieve stellar results. Now I know why. The underlying causes of my orofacial development problems, habitual mouth breathing and poor tongue posture were never addressed.
Now, a decade later, in my mid-twenties, my suboptimal orofacial development not only had always made eating steaks a little challenging, but it was severely impacting the quality of my life because my receded maxilla was not giving enough room for the tongue in my mouth.
My tongue would slip into my airway and deprive my brain and body of vital oxygen at least five times per hour.
In other words, the root cause of my sleep problems was that my face and airways did not develop to their full genetic potential required to accommodate the tongue.
Understanding the root cause of my problems was the first step. The next step was to find a solution.
Dr Teo explained that I would be a candidate for a C-PAP machine, short for Continous Positive Air Pressure, a mask you wear at night to ensure constant airflow.
Essentially, CPAP pushes a continuous flow of air through the mask, and this airflow ensures the airway doesn't collapse on itself even if the tongue rests further back in the airway.
CPAP is a brilliant invention as it saves millions of lives every year.
The problem with CPAP is that it only works if you wear it, and compliance rates with CPAP users are abysmal. The vast majority of people prescribed a CPAP will not use it for even a full year due to discomfort and noise issues.
The other thing is that a CPAP is only a "band-aid-solution", meaning that while it does alleviate the symptoms of obstructive sleep apnea to a very high degree, it does nothing to treat the underlying cause of obstructive sleep apnea, which is the tongue falling into the airway during sleep.
I've never been a "band-aid-solution-guy".
As a personal trainer and wellness coach, I'm more interested in getting to the root of the problem and addressing that with all I've got so that my clients or I can achieve lasting results.
So, CPAP was out of the question.
Next, Dr Teo told me that I would be a candidate for a maxillary advancement surgery. A double jaw surgery where my palatal sutures would be opened and the receded maxilla brought forward where it should be. This would almost certainly improve my sleep quality and the aesthetics of my underdeveloped midface.

That's me in 2012, age 19. People have always called me a baby face. Now, it makes perfect sense why. My maxilla is at the level of a four-year-old. I've desperately tried to make up for the underdeveloped midface with overdeveloped deltoids and arms, and I think I've done a decent job.
Although bringing my maxilla forward to the level of Brad Pitt's sounded good, I decided to give the idea of a double jaw surgery a miss because of the eye-watering financial costs and the fact that no surgery can guarantee results.
The thing about jaw surgeries is that elite-level surgeons are hard to find because the surgery is very challenging and has many possible complications.
Plus, I'd have to wear an orthodontic appliance for a long time before and after the surgery to prepare and stabilise the results.
I asked Dr Teo if we could do the orthodontic appliance without the surgery, and he explained that it would not work in my case without surgery.
My maxilla is so far behind where it should be that it's impossible to achieve that level of expansion and forward translation without surgery because I was already 27 years old.
It turns out that the maxilla stops growing after age 7. Early prevention and intervention are keys to optimal orofacial development and successful orthodontics.
So, we dismissed the idea of a CPAP machine, double jaw surgery and orthodontics. In other words, we decided to avoid invasive treatments and go for a non-invasive solution.
Dr Teo also told me about a splint I could wear at night-time that would advance my mandible (lower jaw) forward. This device is called Mandibular Advancement Splint (MAS, for short).
The benefit of bringing the mandible forward is that it would create more space in my mouth to house my tongue and reduce the risk of the tongue slipping into the airway while I slept.

How The Mandibular Advancement Split (MAS) works.
Even though MAS is also a "band-aid solution", I decided to give it a shot because I was desperate. It was also a bonus that it "only" cost an odd $2000 AUD to get a custom-made splint for my suboptimal orthodontic profile. This was a bargain compared to orthodontics or surgery.
A few weeks after going through a similar experience that had traumatised me as a child, when the mould was taken for the orthodontic appliances I had to wear back then, the splint arrived in the mail.
I was excited and couldn't wait to go to bed that night.
If only I had been able to sleep.
The problem was that even though it worked in the sense that it brought my lower jaw forwards and created more space in the airway, it was uncomfortable as hell.
Although I got somewhat used to it over the subsequent weeks, and it improved my sleep quality, I discontinued the splint after a few weeks because my lower jaw felt really out of whack for the first few hours of the day.
Remember, I already had a recessed maxilla compared to my mandible, so bringing my mandible even further forward only exacerbated my severe crossbite problem. I would feel normal by mid-morning, but eating my breakfast was very uncomfortable.
So, I ditched the splint.
Back to the drawing board.
Orofacial Myofunctional Therapy
A few months passed until, on one of my continuing education Sundays, I stumbled upon an article by an American physiotherapist I followed.
The article was titled:
"Why am I advancing my maxilla at the age of 30".
In the article, the physio shared his own story that sounded exactly like mine.
Suboptimal orofacial development, sleep-disordered breathing problems and a diminished quality of life, and the search for solutions to solve the underlying problem.
The physio explained that, just like me, he was unwilling to undergo double jaw surgery. However, he had found an orthodontist who specialised in orthodontic maxillary expansion for adults.
Again, as I explained before, because adults don't have any skeletal growth left in their jaws, the maxilla can not be expanded safely with an orthodontic appliance.
It is possible to move the teeth forward in the alveolar bone, which may create more space in the roof of the mouth.
However, this is a risky procedure, especially for someone with my profile, because even a little too much movement of the teeth in the alveolar bone will risk severe complications with the gums becoming too exposed.
So, while I read cautiously what the physio was saying about orthodontic appliances for adults, my eye caught something I had never heard of before.
To prepare his orofacial complex for the stress of orthodontics, he had been advised to begin OMT, short for Orofacial Myofunctional Therapy.
Orofacial Myofunctional Therapy is a complementary treatment modality to orthodontics because orthodontists worldwide have realised that unless they address the root cause of suboptimally developed jaws, the orthodontic problems would always return within a few years after a "successful" orthodontic treatment finished.
This was the first time I heard that there were people who call themselves Orofacial Myologists, who specialise in teaching kids and adults optimal tongue posture, swallowing and breathing habits with specific exercises for the tongue, face and upper airway muscles.
The physio reported that since beginning his OMT exercises, he had noticed an almost immediate improvement in his ability to breathe through his nose, and his sleep quality had improved too. He explained that although the exercises were initially designed to teach kids how to hold their tongue in the right place and swallow correctly, they can help adults to strengthen the tongue and the upper airway muscles.
Just like stronger quads, glutes, and hamstrings can propel you forward in space faster, and for a longer time as you run, a stronger and better-conditioned tongue is less likely to fall back into your airway while you sleep to cause obstructive sleep apnea.
Furthermore, because the walls of our upper airways are made of muscles, these muscles could be strengthened too to resist airway collapses while you sleep, further improving airway patency and sleep quality.
The physio was so excited about his results and could see that this had the potential to benefit many of his clients that he did a 4-Day Introduction To Orofacial Myofunctional Therapy - course.
He had written another article about his experiences at the course and outlined the instructions for a few of the exercises he had learned.
I was like: "Damn, this seems almost too simple to be true", but I decided to give the exercises a shot because he did an excellent job at hyping them on the blog.
Giving these simple exercises an honest shot has turned out to be one of the most critical decisions in my life.
After a few days of doing the exercises, I noticed a dramatic improvement in my sleep quality.
Again, just like when I first learned about optimising my breathing habits two years prior when I heard Patrick McKeown talk about it on a podcast, I realised that there was another can of worms that I didn't even know existed.
Excited, I contacted Dr Teo once more to ask if he'd ever heard of OMT and if he knew any excellent practitioners in Melbourne.
Sure enough, Dr Teo had been learning OMT himself at Myofocus in North Melbourne.
There was a brilliant guy called Dr Donny Mandrawa who was an absolute ace regarding airway-focused orofacial myofunctional dentistry. ( Later, I interviewed Dr Donny on my podcast. The episode is titled: Donny Mandrawa - Optimal Oral, Facial And Airway Health 🦷 | Episode 30 )
Without delay, I booked in, and while I couldn't book in with Dr Mandrawa, I was introduced to Dr Hu from Myofocus.
Throughout my visit, Dr Hu kept repeating that he was surprised to see an adult at their clinic. He told me he wasn't sure if their X-Ray machine could be set to my height because most of their patients were kids.
As I said, early prevention and intervention are critical, so if you suspect your child's teeth, jaws, or airways aren't developing to their potential, you should contact an airway-focused myofunctional dentist or orthodontist without delay.
It turns out the machine did work for me, and we completed a comprehensive assessment. The assessment included an X-Ray, photos and functional tests for the tongue.

The initial assessment at Myofocus. We also did a complete dental examination which is not included here.
Dr Hu reiterated what I already knew. My maxilla was at the level of a 4-year-old.
Dr Hu also gave me a basic program of orofacial myofunctional training exercises. These exercises have been designed to strengthen the tongue, facial, and upper airway muscles.
Typically Myofocus sees their new patients weekly to ensure they stay consistent and on the right track. However, since orofacial myofunctional therapy is not covered by Medicare, and my treatment wasn't to prepare for an imminent orthodontic or surgical intervention, we agreed that I'd contact Dr Hu once I felt ready to progress to new exercises.
That appointment was on Wednesday. I went home and got to work.
It only took a few days of consistent practice with the new exercises to notice a dramatic improvement in my sleep quality.
For the first time in a long time, I slept all the way through without waking up a single time. It was a fantastic feeling.
I had to learn more.
The following Tuesday after my appointment, I researched more about Orofacial Myofunctional Therapy when I came across the Australian Academy of Orofacial Myology.
Founded by Rochelle McPherson and Carla Lejarraga, the Australian Academy of Orofacial Myology runs educational courses for dental hygienists, speech pathologists, dentists and orthodontists who want to help their patients establish better orofacial habits (breathing, chewing, swallowing).
I saw that their next 4-Day Introductory Course To Orofacial Myology was due to start in two days, on Thursday. The course was held in Sydney, but because Melbourne was at the height of its world-famous COVID-19 lockdown, they had opened an option to join the class virtually.
I thought that instead of going to Myofocus to get fish for myself, I might as well invest a couple of thousand dollars into the course and teach myself to fish instead.
And sure enough, two days later, I joined a colourful group of dental hygienists, speech pathologists and chiropractors to learn about the amazing world of orofacial myology from two superstar instructors, Rochelle and Carla.

Introduction To Orofacial Myology Course
Day 1/4, 6th of November 2020.
An exercise to elevate and strengthen the posterior tongue and some facial muscles.
It's safe to say that I felt like a fish out of water, and the instructors seemed genuinely surprised that a meathead personal trainer like me had found his way into their course.
The next four days taught me a lot about anatomy above the neck, breathing, sleep-disordered breathing, infant and child development, orthodontic profiles and dental development, to name a few.
Even though I was at a considerable deficit compared to other participants in most of the areas discussed, because of my background in strength and conditioning and biochemistry and biomechanics of breathing through Oxygen Advantage, I could follow and engage with most of the course content.
Most importantly, I could connect the dots between everything I had learned about breathing with Patrick McKeown and how all that was related to the functioning of the tongue and the rest of the upper airway muscles.
I learned that Orofacial Myofunctional Therapy had been proven to reduce sleep apnea events (wake-ups) in adults with moderate to severe sleep apnea (minimum of 15 wake-ups per hour) by a staggering 50%! (Camacho et al 2015)
The results of myofunctional therapy are highly dependent on adherence and patient effort. Therefore, it's more likely that a smaller portion of people who do OMT but put in the work get a much more significant improvement in their sleep apnea scores than those who don't put in the work, and the average benefit happens to be 50%.
This is when I first came up with what I call the holy grail of non-invasive sleep optimisation. The Three Pillars Of Sleep Optimisation are:
1. Sleep hygiene (Week 1 of the Breathe Sleep Perform Program)
2. Breathing efficiency and habits (Weeks 2-6 of the Breathe Sleep Perform Program)
3. Airway patency and tongue strength (Weeks 2-6 of the Breathe Sleep Perform Program)
When writing this in early October 2022, I learned that Rochelle McPherson, the instructor on the course I took, contributed to a recent publication in the Journal of Dental Sleep Medicine titled: Orofacial Myofunctional Therapy For Sleep-Related Breathing Disorders.
"Current literature demonstrates orofacial myofunctional therapy (OMT) decreases apnea-hypopnea index, reduces daytime sleepiness and snoring, arousal index, improvement in quality of sleep and quality of life in both children and adults". (McPherson 2022)
So, when I finished the course in late 2020, I designed a progressive orofacial myofunctional training program and got to work.
My training program had five key exercises, and I invested about 10 minutes daily into my practice.
Soon I became so used to doing these exercises that I would do them unconsciously while reading a book or watching TV.
"Hey babe, I think you look different."
One of the other things I learned in the OMT course was that some adults incorporated these exercises into their life not because they wanted to improve their sleep quality but because they wanted to improve their facial aesthetics.
I'm sure you know that many people inject botox and other expensive chemicals into their faces to enhance their looks with varying results and high risks of negative side effects.
Generally speaking, people like me who didn't realise their genetic potential for jaw development are left with a lot of excess saggy skin on their faces.
The idea with botox and other injectables is to add structure and definition to the face.
It turns out that just like you can develop the size and shape of any muscle in your body, like the biceps, delts, glutes or quads, with progressive resistance training, you can do that with your facial muscles too.
Orofacial myofunctional exercises involve isometric and isotonic contractions. Isometric means holding a particular position and resisting gravity or pushing into an immovable object, and isotonic implies that movement is involved.
However, since you can't curl dumbbells with your tongue or cheek muscles, the best you can do in most cases is to train these muscles with isometric contractions against the pull of gravity.
Because there are zero external loads on most myofunctional exercises, the amount of mechanical tension, which is the primary driver of muscle hypertrophy, is minimal.
However, as you discover very soon after trying the isometric exercises, there is some muscle tension, albeit very little. Some blood and metabolite build-up must occur because you can get a "pump" on your facial muscles or the tongue just like you can get a "pump" on your biceps or glutes.
So, in theory, as long as you build enough time under tension with the orofacial myofunctional training exercises, you might see some hypertrophy in your facial muscles.
In turn, the structure and definition of your face may improve as a result.
I knew about this, but since my primary motivation for my OMT practice was to improve my sleep quality, most of the exercises I included in my program were for the tongue and the upper airway muscles, not facial muscles.
To be completely honest with you, I was sceptical that I could make noticeable changes to my facial profile.
However, because I had decided to document my journey, I kept taking progress shots similar to the ones Dr Hu took of me during my visit to Myofocus in November 2020.
Every month, I would ask Theresa to take photos of my face.
On one of these occasions, after three months of practice, as she was comparing the photo angles to the previous photos to ensure she was taking a picture of the same view, she said: "Hey babe, I think that you look different".
I put the photos next to each other with a mobile app.
![]()
3 Months before/after progressive orofacial myofunctional training
Holy shit. I looked different.
I couldn't put my finger on what it was, but somehow I looked healthier.
My eyes looked brighter, and I looked more energetic.
This was an exciting boost to my confidence, and I started pouring even more effort into my daily practice.
I worked until I achieved an unbearable pump in my tongue and cheek muscles daily. The progress was slow, but it became more and more apparent from month to month.
Because I had seen some results myself, I started searching online to see if other people had been able to create a visible transformation in their facial aesthetics with orofacial muscle training.
While I was able to find some before/afters of people who claimed they'd done OMT, I came across mostly "mewing" before/afters.
I first learned about "mewing" when I read James Nestor's book: Breath, The New Science Of A Lost Art.
The term "mewing" was coined after Professor John Mew, a revolutionary English orthodontist who gained a lot of early hate among other orthodontists because of his controversial views about the origins of malocclusions.

Professor Mew and some extraordinary life-changing results with his patients. I wish my parents had taken me to see someone who practised his principles when I was a kid.
Professor Mew was the first to put forward the idea that most malocclusions originate from deficient jaws. The development of the jaws drives the show and determines how teeth will erupt and what one's face looks like, and how big the airway is.
So, to fix someone's occlusion and achieve a harmonious facial profile, you had to get their jaws growing.
And what drives the show regarding the development of the jaws?
According to Professor Mew and most modern airway-focused orthodontists and dentists, and orofacial myologists, the tongue does.
See, before the growth spurt in early childhood, the bones of the face and jaws are incredibly malleable.
So malleable that the resting position of the tongue and the tongue's action during the action of swallowing exerts pressure against the maxilla, the top jaw, and encourages the maxilla to grow outwards and forwards.
![]()
Another image courtesy of Professor John Mew. According to the book "Jaws - The Story Of A Hidden Epidemic" which is a brilliant book written by two Stanford Professors, Ehrlich and Kahn, this boy who had normal development at age 10 became a mouth breather because he developed nasal congestion because he was allergic to the family's new pet gerbil. By age 17, the unfortunate results of mouth breathing on his facial profile are clearly visible.
The other benefit of holding the entire tongue against the roof of the mouth is that the posterior aspect of the tongue creates the floor of our nasal cavity.
When the back portion of the tongue is elevated into this position, it creates space in the airway during wakefulness and sleep. It will become easier to breathe through your nose when you figure out how to elevate the back portion of the tongue on the roof of the mouth. (Easier said than done for beginners).
On the other hand, if the tongue is on the floor of the mouth, the airway space diminishes as the tongue rests further back in the airway. This makes nasal breathing harder during the day and increases the risk of snoring and obstructive sleep apnea at night.
Somewhere along the way, the term "mewing" emerged to describe the action of holding one's entire tongue against the roof of the mouth.
In other words, "mewing" simply means holding one's tongue in the anatomically most advantageous position that instantaneously improves your nasal breathing ability.
Interestingly, many adults claim online that they've been able to grow their jaws, particularly their maxilla, by "mewing".
As someone with a deficient maxilla, this caught my eye a long time ago. Still, the theory contradicts the timeline of skeletal development of the human head I had learned in the Introductory Course To Orofacial Myofunctional Therapy - Course, and from interacting with Dr Teo and Dr Hu.
The maxilla will not grow without an orthodontic intervention after age 7, and even with orthodontics, it might be too late if you are in your mid-teens. Once again, early intervention is vital.
So, to see literally hundreds of very impressive before/after photos online, I was sceptical.
Remember, people are very good at photoshop these days.
I couldn't find a single before/after with a legitimate before/after X-Ray analysis to go with it.
Then I thought to myself... Wait a minute. Dr Hu took X-Rays of me in November 2020 on my visit to Myofocus!
What if I went and did another round of photos and X-Rays with Dr Hu to objectively quantify whether or not I had been able to grow bone in my face or not?
Second trip to Myofocus
On the 10th of December 2021, about 13 months after my initial visit to Myofocus, Dr Hu once again adjusted the X-Ray machine to fit his oversized patient that day.
I could tell he was genuinely surprised to see me return and request another round of photos and X-Rays.
We did another entire battery of photos and functional tests, and a few days later, he invited me for another visit to review the results.
He explained that he had done another Jefferson Analysis, a technique used to evaluate lateral cephalogram radiographs (X-Rays of the side of the head), and there was a small but insignificant difference between the positions of the maxilla and the mandible between the new and initial X-Rays.
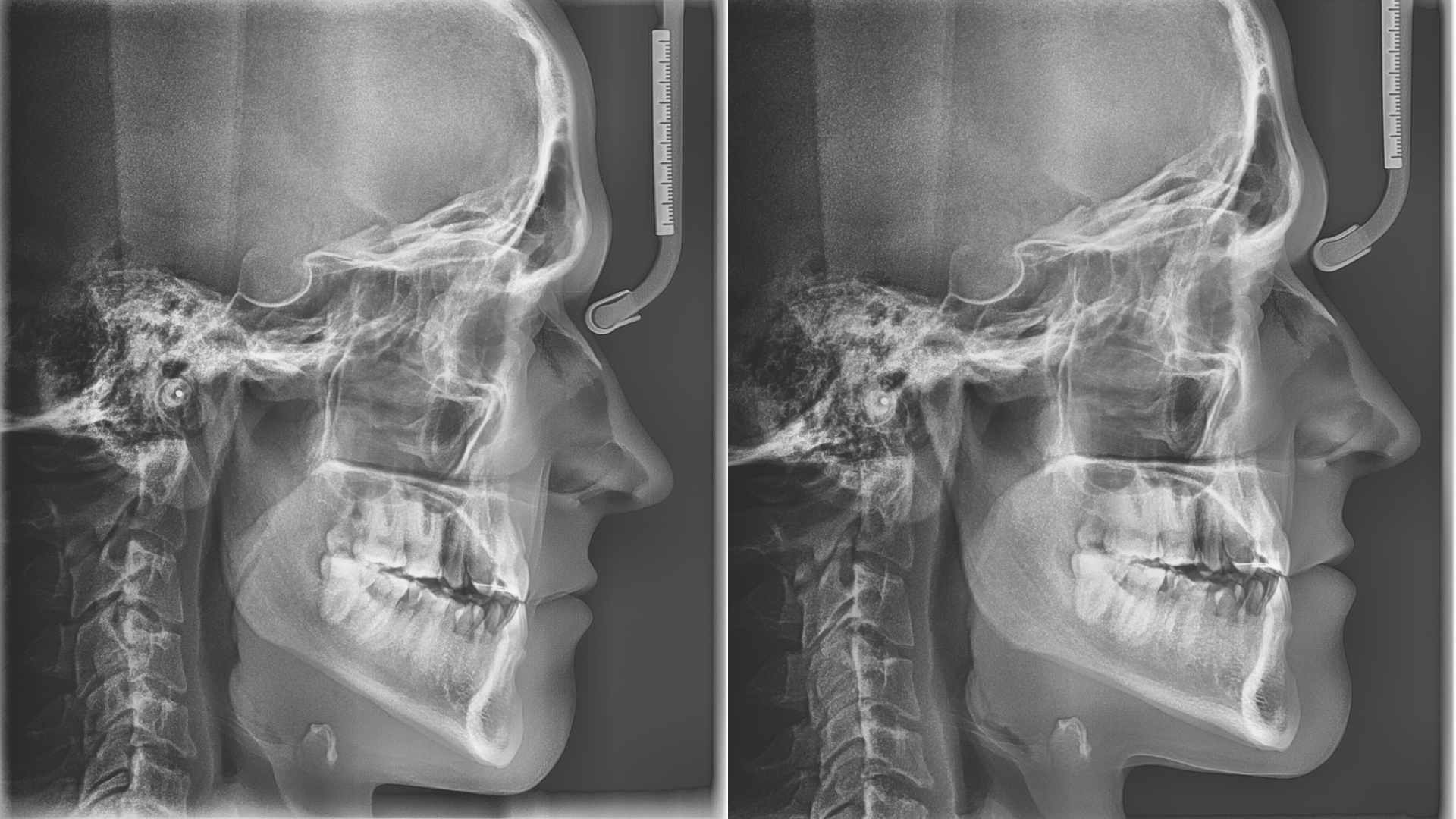
Before vs After. Looks the same to me, apart from a small difference in the angle of the head. Can you spot any difference?

According to the Jefferson Analysis, which analyses the image by identifying critical landmarks in the facial profile, my maxilla had moved forwards 0.6mm, and my mandible had moved backwards 1.1mm. This is most likely due to the difference in the head position.
He also pointed out that, unfortunately, we weren't able to get the image quite right, and there was a slight difference in the tilt of my head, which could account for some of the differences in the positions of the bones.
Slightly disappointed, I went home that day and put the photos we took of me next to each other on Canva.
Holy shit. It worked. I looked better.
![]()
13 Month Progressive Orofacial Myofunctional Training before/after.
My eyes looked sharper, my skin was tighter across my face, and it looked like I'd had a botox injection on my cheekbones. I looked much more alert than before.
Overall, my face had more structure and definition, and even my jaws looked slightly more defined.
I was thrilled, but this only raised more questions.
What could explain the results?
If "mewing" worked, there should have been a significant change in the size or position of my maxilla.
But there wasn't.
The only plausible explanation I have is that a combination of increased muscle size due to progressive strength training of my facial muscles and improved sleep quality had transformed the way my face looked for the better.
I decided to create a Youtube video where I go over the X-Ray analysis results and the before-after photos. I titled it with this clickbaity title: "Does Mewing Really Work For Adults? 13-Month X-Ray Before/After Analysis".
The clickbait worked.
When writing this, there have been more than 30000 views, 1200 likes, and 300 comments from people desperately looking for proof that mewing can improve their facial aesthetics.
Not exactly viral, but it proves that many people are out there looking for solutions.
I'm genuinely touched by how many people took time out of their lives to comment on the video and share their own experiences.
However, the thing that's driving me mad is that most people who commented didn't actually watch the entire video or listen to a word I said.
Here are some of the most liked comments that show the gist of it:
"damn man, crazy differences! never expected that somebody your age would improve his facial aesthetics so much through mewing. very impressive, especially your eye area has improved a lot. i've been mewing for 4 months now - fingers crossed i'll be having similar results like you ;)"
"I'm 41. I've been mewing since 2019 and i also had Invisalign in 2020. My face has changed massively and i look like 30. Lots of people asked me if I had surgery or fillers cause i have such a youthful look".
S#it! You didn't even watch the video!
I just showed you evidence that mewing did NOT work in the way you think because there was no significant change in the size or position of the maxilla or mandible!
What you are looking at are the side effects of progressive orofacial myofunctional training to improve your sleep quality and breathing efficiency.
I'd recommend watching the video for yourself to see the detailed analysis for yourself.
She Said Yes!
![]()
6.8.2022 at the top of Ukko Koli, Finland
Four years later, after Theresa and I moved together in 2018 and first discovered each other's breathing and sleep problems, we got engaged while on a trip to my home country, Finland.
I honestly think we would not have made it this far if we hadn't found the solutions to our problems.
We are forever grateful to everyone who we were able to learn from along the way.
I'm also grateful to you that you've made it all the way this far into the very end of the article.
I hope that it's come across how important and life-transforming this journey has been for me, mentally and physically, and it's been great to share the journey with you.
Third Trip To Myofocus (Updated 24th of March 2023)
I promised you I would keep going to Myofocus to update the shots once per year, and I did.
![]()
Continued progress has been made! Watch out, Brad Pitt!
Here is the updated before/after analysis video:
I'm thrilled to let you know that not only have I made progress with how my face looks, but my sleep quality has also continued to improve steadily.
Let's keep it going.
I'm Not a Therapist
I want to clarify that I'm not an orofacial myofunctional therapist.
I do not prescribe therapy, treatments or diagnoses for any medical conditions.
I'm just a curious strength and conditioning coach who loves diving deep into a topic I'm interested in. Nothing is more interesting to me than performance, sleep, health and longevity.
I have compiled all the OMT tools and methods I've used to achieve these sleep quality and aesthetic results you've just read about.
I have combined all that with the breathing tools I've learned over the last few years to reduce stress, prime the body for a great night's sleep, increase stress tolerance, unblock the nose and focus the mind.
Then I've sprinkled some strength and conditioning principles and exercise science to ensure that the programs are progressive and logically sequenced.
Finally, I've added all the sleep hygiene strategies known to man in easily digested and understandable videos.
![]()
These are the ingredients from which the Breathe Sleep Perform program has been baked, and I'm very proud of the finished product.
I know that it is truly a unique experience because nobody else on this planet has had the same journey as I have.
I would love you to join me on the six-week program to deliver all the tools I've accumulated over the years in a logical order.
Your sleep quality is guaranteed to improve within six weeks.
However, you won't achieve a similar aesthetic transformation in as little as six weeks.
I've worked hard and consistently, and I doubt anyone can be as diligent with their practice as I am.
However, you will be armed with the same tools I've used, and you'll get to ask questions directly from me.
So, I'm here for you if you are willing to do the work.
If you don't like the course, you will get your money back through the 14-Day comfort guarantee with no questions asked.
Thank you for reading all the way through. You are a champion.
I hope that I'll see you in the program.
This is Coach Pyry,
Let's do this.
Ready to unleash your potential through muscle building, strength, health and sustainable fat loss?
Get in touch via the form below, and we'll book your discovery call to map out your personalised plan to your best shape ever.
